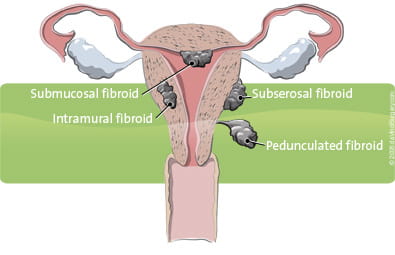
At least one-quarter of all women will have uterine fibroids at some point in their lives.1 These benign (non-cancerous) tumors can grow underneath the uterine lining, inside the uterine wall, or outside the uterus, with many women experiencing no symptoms at all. In some cases, however, uterine fibroids can cause excessive menstrual bleeding (also called menorrhagia), abnormal periods, uterine bleeding, pain, discomfort, frequent urination, and infertility.2
The most common treatments for fibroids include uterine fibroid embolization, which shrinks the tumor, and surgery which most often involves removing the entire uterus through a hysterectomy.3
While a hysterectomy is a proven way to resolve fibroids, it may not be the best surgical treatment for every woman. If, for example, you hope to later become pregnant, you may want to consider alternative treatments such as a myomectomy which preserves the uterus while removing the uterine fibroids.
Each year, roughly 65,000 myomectomies are performed in the U.S.4 The conventional approach to myomectomy is open surgery, through a large abdominal incision.5 After each uterine fibroid is removed, the uterine wall must be carefully repaired to minimize potential uterine bleeding, infection, and scarring. Proper repair is also critical to reducing the risk of uterine rupture during future pregnancies.
A myomectomy may also be performed laparoscopically; however, this approach may compromise the results compared to open surgery.6 Laparoscopic myomectomies are often more challenging and take longer than open abdominal myomectomies, with up to 28% being converted to an open abdominal incision during surgery.7
Fortunately, a robotic myomectomy combines the best of open and laparoscopic surgery. With the assistance of the da Vinci Surgical System—the latest evolution in robotics technology—uterine fibroids can now be removed through a few small incisions with unmatched precision and control.
If you have been diagnosed with uterine fibroids, we will work with you and your primary care physician to determine the right treatment option that will ensure you receive the best possible outcome.
1. Newbold RR, DiAugustine RP, Risinger JI, Everitt JI, Walmer DK, Parrott EC, Dixon D. Advances in uterine leiomyoma research: conference overview, summary, and future research recommendations. Environ Health Perspect. 2000 Oct;108 Suppl 5:769-73. Review.
2. National Institutes of Health: Fast Facts about Uterine Fibroids.
3. Becker ER, Spalding J, DuChane J, Horowitz IR. Inpatient surgical treatment patterns for patients with uterine fibroids in the United States, 1998-2002. J Natl Med Assoc. 2005 Oct;97(10):1336-42.
4. Lumsden MA.Embolization versus myomectomy versus hysterectomy: Which is best, when? Hum Reprod. 2002; 17:253-259. Review.
5. Becker ER, Spalding J, DuChane J, Horowitz IR. Inpatient surgical treatment patterns for patients with uterine fibroids in the United States, 1998-2002. J Natl Med Assoc. 2005 Oct;97(10):1336-42.
6. Kristen A. Wolanske, MD; Roy L. Gordon, MD. Uterine Artery Embolization: Where Does it Stand in the Management of Uterine Leiomyomas? Part 2. Appl Radiol 33(10):18-25, 2004. Medscape.10/27/2004.
7. Advincula AP, Song A, Burke W, Reynolds RK. Preliminary experience with robot-assisted laparoscopic myomectomy. J Am Assoc Gynecol Laparosc. 2004 Nov;11(4):511-8.